Skin Problems and Menopause
Skin Problems and Menopause
Many women experience skin problems during menopause, because the hormone oestrogen declines and with it our skin plumpness and elasticity. Lower Oestrogen can also cause excessive wrinkles, flushing, dryness and impaired wound healing. Moreover, oestrogen may even play a role in protecting the skin from the sun’s harmful UV rays so less of it can have many far-reaching consequences. Other skin problems such as irritation, sensitivity, breakouts or dryness can be caused by hormone imbalances common at this time and is often made worse by additional menopause symptoms like hot flushes, night sweats and poor sleep.
In this blog you can learn WHY you might be experiencing hormonal skin problems right now and WHAT you can do about it.
What causes wrinkles?
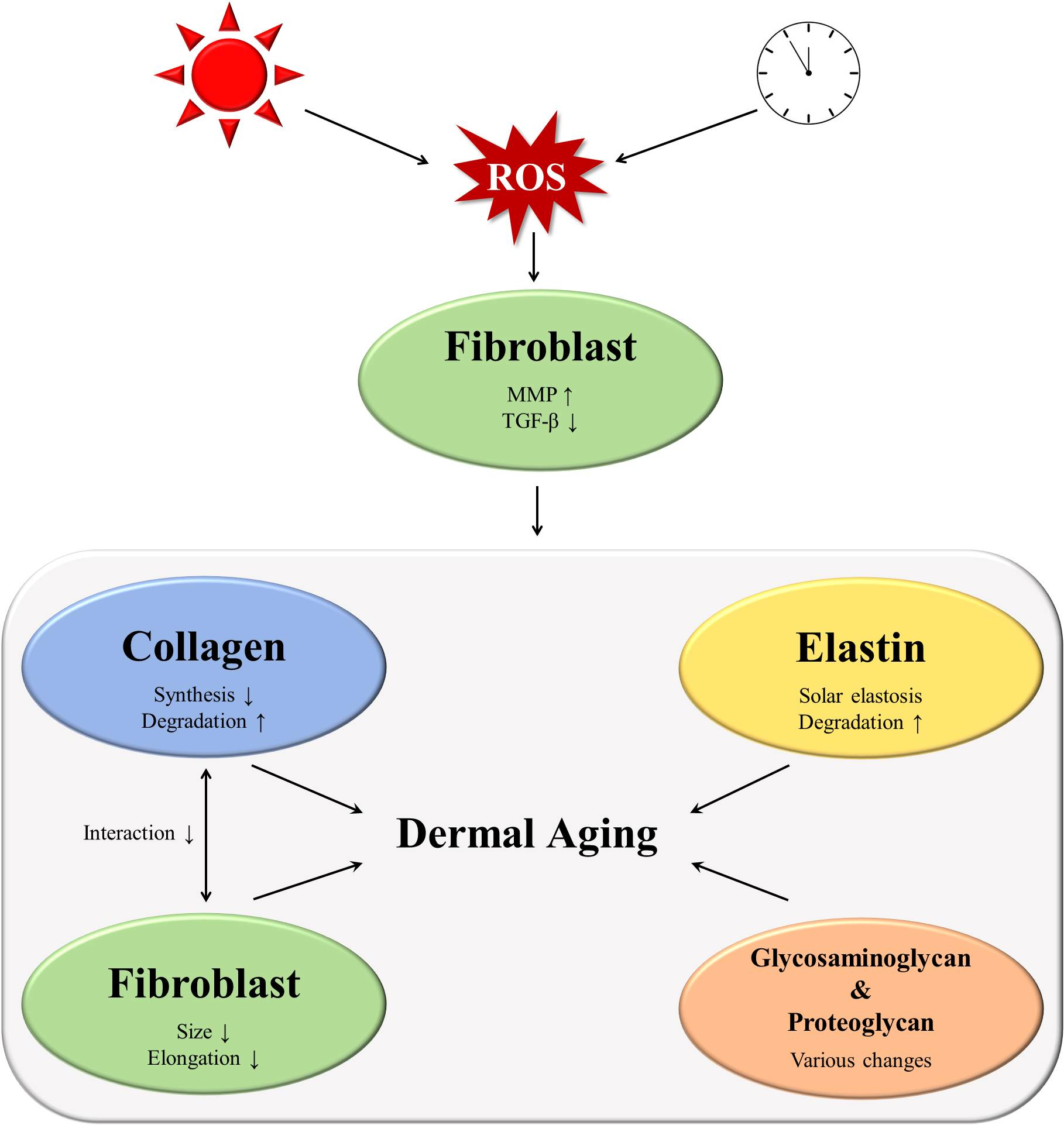
Collagen is a protein that gives skin its firmness and elasticity and makes up about 80% of adult skin. It is at its highest when we are born, and it decreases in adulthood. Ageing, particularly wrinkling and sagging increases post menopause because shockingly up to 30% of collagen is lost in the first five years after menopause. Much of this is due to increased oxidative damage from free radicals. Read more.
The science bit, or skip to next bit
To understand the knock-on effects of collagen we need to know a bit about the skin dermis that lies beneath the visible epidermis. The skin dermis is made up of the ‘extracellular matrix’ (ECM.) At its best the matrix looks a bit like a good mattress! It makes your skin plump and bouncy. It has many components, with collagen being a major part. The elasticity is attributed to elastin, a protein that coils and recoils like a spring within the elastic fibres of the skin. Additionally, there are Glycosaminoglycans (GAGs). You may have heard of some like hyaluronic acid and chondroitin sulfate in skincare and joint supplements. They are water-binding molecules that can hold nearly 1000 times their own weight in water. This provides moisture for the skin matrix, giving the skin suppleness and making it resilient. (2)(3).
Skin problems at menopause
Synthesis of collagen and elastin proteins is partly controlled by oestrogens and their decline means a reduction of not only elastic fibres but also water holding molecules (GAGS). This is because of the interdependence of the dermal components. This two way relationship means they help support and maintain collagen, elastin and fibroblasts that synthesise collagen. Therefore, reduced collagen and elastin has a knock-on effect that hinders the interaction between all these building blocks of the dermis. These functions explain why we may experience some unpleasant effects on the skin around menopause.
-
Thinning of the skin
The reduction of protein synthesis and resulting loss of collagen and elastin cause loss of skin volume and elasticity. Because of this the dermis starts to thin due to the loss of collagen, GAGs and water causing it to be much more prone to bruising and tearing. This can exacerbate other menopause related skin problems.
-
Slow wound healing
The skin becomes thin and fragile, making it susceptible to bruises and injury. Low oestrogen is also thought to contribute to poor wound healing. Subsequently there is a significant difference in recovery time between pre and postmenopausal women and this tells us that hormones are playing a bigger role in wound healing than chronological age. (4)
-
Dry Skin
A common problem in menopause is dryness. As mentioned, skin hydration is supported by production of GAGs, which hold water in the skin. However, dryness relates to lack of oil or sebum. Oestrogen plays a part in sebum production, which keeps skin lubricated, provides antioxidants and protection from light, bacteria for the skin. It supports immunity and has pro- and anti-inflammatory function. When reduced at menopause it disrupts the barrier function, decreasing water retention increasing transdermal water loss. Some women experience Pruritus (skin itching) due to this extreme dryness. (1) (4) This also leaves the skin more open to irritation and sensitivity. Unfortunately, sebum may also promote normal collagen production.So it is important to nourish your skin topically.
-
Skin redness and sensitvity
As many as 50% of women going through menopause have hot flushes and or night sweats and this causes skin flushing and redness. The cause of hot flushes is not completely understood. However they occur due to decreased oestrogen levels that cause the body’s thermostat in the brain (hypothalamus) to become more sensitive to slight changes in body temperature affecting the skin’s microcirculation. This may make the skin more prone to dilated capillaries, and broken veins causing flushing to last longer than the hot flush. Finally, Rosacea can be a complication of this and is often miss understood. (5)
-
Acne
Both dry and oily skin can happen at perimenopause. Spots at 50 are common! Hormonal spots are common at any age in response to the hormone disruption during the menstrual cycle. So fluctuating hormones in perimenopause may cause a similar effect. Spots are mainly due to increased androgens that upregulate the sebum production. Some forms of hormone replacement therapies (HRTs) may also trigger breakouts initially, because of the hormones it introduces. There are many underlying causes of Acne and Acne rosacea so nutritional approaches are often best alongside the correct topical products. (6)
Nutrients to Nourish Menopause Skin
Essential Fatty Acid Omega 3
Omega 3 has much research; it contains docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). These two essential fatty acids have powerful anti-inflammatory and healing properties. For different skin concerns including oily skin conditions and protects against sun damage. They boost skin hydration and improve the fatty acid barrier of the skin, which helps reduce water loss, and resolve dryness-related skin itching. It has been shown to improve symptoms of psoriasis. Dry skin can be due to a lack of fats in the diet, often related to a low- fat diet or one lacking the ‘healthy fats.’ These include olive oil, coconut oil, avocado. Omega 3 is found in oily fish like salmon, mackerel, anchovies, sardines, or herring.
Vitamin D
Vitamin D has an integral role in skin barrier function and skin cell growth. It is key for maintaining the skin immune system, the first line of defence against harmful pathogens. Keratinocytes in the outer layer of the skin, are the only cells in your body that can form vitamin D. Low vitamin D is associated with dry, itchy skin disorders including eczema and psoriasis. There is also a correlation between vitamin D and skin moisture. Do discuss with your supplementation healthcare provider.
Vitamin D from the Sun
The main source of Vitamin D is the sun. Only exposure between April and September in the UK provides sufficient year-round vitamin D. The timings minimise the risks of sunburn and skin cancer.
Sun exposure recommendations
- Caucasian skin types –10-15 minutes exposure
- Darker skin types, 25-40 minutes exposure
Other sources include oily fish as above, red meat, egg yolks and chestnut mushrooms exposed to UV light.
Vitamin C
The skin contains very high levels of vitamin C and it may improve many factors of skin health. Known as a powerful, skin-protective antioxidant and essential for collagen production, it is key for skin structure and moisture. Vitamin C in combination with other nutrients has been shown to significantly improve skin conditions and hydration as it may enhance skin barrier function, reducing water loss and preventing dehydration. Good sources are green leafy vegetables, red peppers, and green peas!
Ceramides and hyaluronic acid
Some research shows that ceramides may increase skin hydration and support plump skin, they are a type of fat that naturally occurs in the skin and diminishes with age and hormone changes. They form the mortar of your skin barrier between the skin cells holding it together and preventing water loss. They provide hydration and moisture that keeps your skin supple, and comfortable. Similarly, Hyaluronic acid helps hold water in the dermis of skin, having a plumping moisturising effect. You can effectively use this topically on the skin. Ceramides are found in soybeans, eggs, dairy, wheat germ, and brown rice. Whilst soya assists in Hyaluronic Acid synthesis, and it is found in citrus fruits, tuber & green Vegetables, nuts and Seeds
In conclusion
To conclude, understanding what’s happening to our skin in perimenopause can help us to take care of our skin both nutritionally and topically. It can help us accept a level of change and also support us to regain long lost confidence. I hope it empowers you to make some adjustments. Thisis why I love to providing insight into foods, lifestyle changes and topical products that can support skin health, help you look your best. (8)
As a nutritionist and skin therapist it is my mission to inspire women to find their menopause mojo by nourishing themselves inside and out to restore vitality.
If you’d like to find out how I can help you personally book a free discovery call.
You can share how your skin has been changing and challenging you over time and I will let you know how I can best meet your needs. My services include both nutritional therapy and skin treatments. Within each I offer different levels of bespoke nutritional advice to meet your needs.
August special offer save £10 on The Environ Facial until the end of August. Inclusive of a skincare consultation.
REFERENCES
1.Calleja-Agius J, Brincat M. The effect of menopause on the skin and other connective tissues. Gynecological Endocrinology [Internet]. 2012 [cited 2020 Nov 19];28(4):273–7. Available from: https://www.tandfonline.com/doi/abs/10.3109/09513590.2011.613970
2. Shin JW, et al. Molecular mechanisms of dermal aging and antiaging approaches. International Journal of Molecular Sciences [Internet]. 2019 May 1 [cited 2020 Nov 19];20(9). Available at: https://doi.org/10.3390/ijms20092126
3. Farage MA, et al., Skin, mucosa and menopause: Management of clinical issues. Skin, Mucosa and Menopause: Management of Clinical Issues. Springer Berlin Heidelberg; 2015. 1–509.
4. Nair P. Dermatosis associated with menopause. Journal of Mid-life Health [Internet]. 2014 [cited 2020 Nov 19];5(4):166. Available from: /pmc/articles/PMC4264279/?report=abstract
5. Duffy OK, Iversen L, Aucott L, Hannaford PC. Factors associated with resilience or vulnerability to hot flushes and night sweats during the menopausal transition. Menopause: The Journal of The North American Menopause Society [Internet]. 2012 Dec [cited 2019 Apr 11];20(4):1. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23250082
6.Bhate K, Williams HC. Epidemiology of acne vulgaris. Vol. 168, British Journal of Dermatology. 2013. p. 474–85.
7.Fisher GJ, et al. Pathophysiology of Premature Skin Aging Induced by Ultraviolet Light. New England Journal of Medicine. 1997 Nov 13;337(20):1419–29. https://www.nejm.org/doi/full/10.1056/nejm199711133372003
8. Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: A review. Vol. 30, International Journal of Cosmetic Science. 2008. p. 87–95. https://doi.org/10.1111/j.1468-2494.2007.00415.x